Treatment of Facial Paralysis


What is facial paralysis
Facial paralysis occurs when a person is no longer able to move some or all of the muscles on one side of the face because of nerve damage. Your facial muscles droops or become weak.
This condition typically caused by:
- infection or inflammation of the facial nerve
- head trauma
- head or neck tumor
- stroke
Facial paralysis can come on suddenly (in the case of Bell’s palsy, for example) or can happen gradually over a period of months (in the case of a head or neck tumor). Depending on the cause, the paralysis might last a short or extended period of time.

Facial palsy
Facial palsy is condition in which there is lesion of the facial nerve and the resultant paralysis in the muscles that it supplies.

Bell's palsy
This is a common acute, isolated facial nerve palsy believed to be due to viral infection (most probably herpes simplex) that causes swelling of the nerve within the petrous temporal bone. Facial palsy can be upper and lower motor neuron, while Bell's palsy is typically acute lower motor neuron paralysis, uni or bilateral. Usually idiopathic, but also can be associated with intermittent HSV reactivation. It is usually mononeuropathy compared to facial palsy may be associated with multiple cranial nerve involvement depending upon lesion.

There will be following features on the side of lesion:
Loss of facial expression.
Drooping of the face- Low eyelid, eyebrow and corner of mouth sag.Closing the eye is difficult.
Eating is difficult because food collects in the side of the cheek and fluid seeps out of the corner of mouth.
Speaking, whistling and drinking are impaired.
Non-verbal communication is lost as the patient
cannot register the pleasure, laughter, surprise, interest and worry.
The patient tends to sit with the hand over the side of face.

MANAGEMENT
Spontaneous recovery occurs toward the end of
second week. Thereafter, continuing recovery occur. Fifty percent recover
within three months. Continuing recovery may take 12 months to become complete.
About 15 percent of patients are left with a severe unsightly residual
weakness.
Medical
Steroids (prednisolone 60mg daily reducing to nil
over 10 days).
Acyclovir for viral infection.
If there is severe residual paralysis, cosmetic surgery and/or reinnervation (nerve anastomosis of the lingual to the facial) are some times performed after a year has been elapsed.

Physiotherapy
During the paralysis:
The selection of the suitable physical agent
depends upon the experience or the choice of an experienced physiotherapist.
Physiotherapist may choose from a number of physical agents available.
Ultrasound (Ultrasound therapy)is given
over the nerve trunk in front of the tragus of ear and in area between mastoid
process and mandible. There is no fear of applying ultrasound while doing the
treatment of patient with Bell's palsy. The ultrasound is always applied on the
side of lesion in front of the tragus of ear & in area between the mastoid
process and mandible where the maximum tenderness of the facial nerve is
determined by palpation. It is applied in slow circular motion with a starting
dosage of 1 watt per square centimeter for 10 minutes. The dosage may be
increased on the subsequent sessions if no remarkable improvement is noted. Let
me explain that ultrasound waves cannot traverse the bone. That means
ultrasound has zero penetration in the bone. Infact, ultrasound waves are
reflected away from the bone. So there is no fear in applying the ultrasound on
face. (This is only for LMN lesion type)

Low level laser therapy (infrared
808 nanometer wavelength 400 mill watt power for 5 minutes continuous)

Infra-red: Infra red may be applied to warm the muscles and improve the function, but you must ensure that eyes are protected with linens when you are applying infra-red to face. Timing should be for 10 to 20 minutes at a distance usually between 50 and 75 cm or more depending upon the instrument used.

Ultraviolet Therapy: Formerly ultraviolet was frequently used to give third or fourth degree erythema doses over the facial nerve trunk and in area between mastoid process and mandible (at the point of emergence of facial nerve on face)to combat the infection and inflammation. The type of lamp used for this type of treatment is the Kromayer lamp. The Kromayer lamp is a water cooled mercury vapor lamp which eliminates the danger of infrared burn. It has the advantage that it can be used in contact with the tissue or with suitable applicator it can be used to irradiate a suitable body cavity.
Testing the dosage can be done with Kromayer lamp
in contact with the skin, so very small holes are used, e.g. 0.25 square cm.
since exposure time need only be very short. It is often useful if the Kromayer
lamp has standard dosage time recorded on it for contact and 10 cm. The front
of the Kromayer lamp is cleaned with an appropriate solution and when it has
had its full 5 minute warming up period the lamp is ready for use. The front of
the lamp is held as close as possible to the skin or the target tissue. At
least an E4 dosage is given. Treatment could infact be given at a set distance
of, say 4 cm.
Microwave diathermy: As far as
micro wave diathermy application is concerned, there is strict contra
indication for the use of micro wave diathermy for the treatment of face as
micro waves can spread randomly and can damage the lens of eye causing the
opacity of the lens. So there is no room for the application of micro wave to
face.

Short Wave Diathermy: SWD can
be safely applied for the treatment of facial palsy at the point of emergence
of nerve on the face. The technique used may be monopolar or bi polar. In
bipolar technique using the capacitor field method or induction or cable
method, the one facial mask electrode is used as an active electrode for
applying the rays to face while the second or indifferent electrode used on
some distant part of the body (usually cervical or dorsal spinal area) to
complete the circuit. In monopolar electrode method only one electrode is used
to direct the rays to the target treatment area site and no second electrode is
used at all. The treatment time is between 10 and 30 minutes. Shorter sessions
are used for mild conditions. Treatment is given on daily basis to produce the
required results.

Electrical Stimulation: The only
form of electrical current used on face is interrupted direct current (I.D.C.)
whether or not there is reaction of degeneration. This is requested only to
preserve the bulk of facial muscles and to prevent their atrophy while waiting
them to be in function whenever their re innervations arrives in case of axotomesis
or reconduction after neurapraxia if the nerve is not damaged completely. There
is no room for the use of faradic current use on the face as it could lead to
cause secondary contractures of the face. Moreover, most patients find it
intolerable on face due to its unnecessary uncomfortable sensory stimulation.
This is due to the reason that the faradic current has a frequency of 50 cycles
per second, and so produces the tetanic contraction of the muscles that it
stimulates. Although for muscle contraction faradic current is surged to
produce alternate contraction and relaxation yet the tetanic type of
contraction produced by these 50 pulses delivered in just one second, is not
required on face. The face muscles are very thin and delicate and could not tolerate
this tetanic type of contraction and may be damaged to produce the secondary
contractures. If secondary contractures are produced, all form of electrical
stimulation should be abandoned temporarily to avoid further damage to the
muscles. The face should be gently stretched and massaged.
Heliotherapy: Following the traditional way by using the convex lens to focus the sun rays to produce the third or four degree erythema dosages to facial nerve trunk and in area between mandible and mastoid process behind the ear and it frequently give dramatic result with excellent recovery of facial palsy. The treatment was needed to repeat after one week to repeat the same session of the dosage. Only three or four sessions of this kind were needed to do the excellent management of the patient. In fact, it is one kind of heliotherapy treatment which is available from the natural source of power i.e. the sun. The sun rays are a mixture of infra red rays and ultraviolet rays and visible rays on the electromagnetic spectrum. The thermal effect is produced by the infra red portion of the sun rays while the chemical effect like tanning of skin, effect on photographic film, formation of vit. D is due ultraviolet portion in the sun rays. The visible rays which are near to infra red portion on the electromagnetic spectrum produces effects similar to infra red rays. The visible rays which are near to ultra violet portion on an electromagnetic spectrum produces effects similar to ultraviolet rays. The erythema formation is due to ultraviolet portion of the sun rays. Usually fourth degree erythema dosage is required to produce the required therapeutic results.


Iontophoresis: Zinc,
potassium iodide or chloride iontophoresis is given to the affected ear to
treat the otitis media if there is infection of the middle ear.
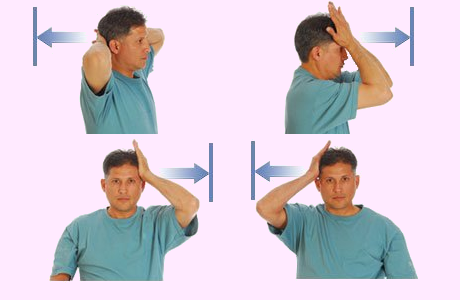
Massage: The patient derives great benefit from the massage. Massage may be taught to the patient.Stroking in the upward, outward direction. It is given from chin upwards to the temple and from the middle of forehead downwards towards the ear. The technique should be gentle but at the same time stimulating.Slow finger kneading applied over the paralyzed muscles maintains skin suppleness and muscle elasticity. Small circular finger kneading can be given all over the affected side of the face, care being taken not to stretch the muscles. Tapotement may be administered in the form of tapping quickly and lightly with the finger tips. It must be done very gently over the forehead and superficial ridges, where only a thin layer of muscle covers the bone.Frictions are given at the point where the nerve enters the face to soften any inflammatory deposit.Vibrations performed with the tip of one or two fingers can also be used over nerve trunk at this point or they may be administered by placing the whole flat hand on the affected side of face.These techniques applied daily for 5 minutes or so help to maintain lymphatic and blood flow and prevent contractures.

Taping : Application of adhesive tape-elastic or non-elastic, in order to provide support and protection to soft tissues from further injury in the functional position.

.jpg)
Comments
Post a Comment